Advancing heart disease diagnosis – influencing international guidelines and commercial adoption of automated ECG analysis software
Submitting Institution
University of GlasgowUnit of Assessment
Clinical MedicineSummary Impact Type
TechnologicalResearch Subject Area(s)
Medical and Health Sciences: Cardiorespiratory Medicine and Haematology, Clinical Sciences, Neurosciences
Summary of the impact
The electrocardiogram (ECG) is one of the most commonly used medical
tests which assist in
diagnosing heart disorders worldwide. However, diagnosis relies on
accurate interpretation of ECG
recordings. Studies by University of Glasgow researchers have led to
changes to international
guidelines for ECG-based diagnosis of a heart attack (myocardial
infarction; MI) and have led to
significant refinements to the automated ECG analysis software called the
`Glasgow Program'.
Commercialisation of the Program since 2008 has resulted in its
incorporation into some of the
market-leading medical devices, with approval of the Glasgow Program by
the FDA and more than
40,000 devices sold worldwide, potentially aiding millions of patients
around the world. The
Program assists hospital doctors, family practitioners and others such as
first responding
emergency services, e.g. ambulance and fire services, with the reliable
interpretation of ECGs,
enabling rapid and accurate diagnosis and treatment of patients with a
variety of heart problems.
Underpinning research
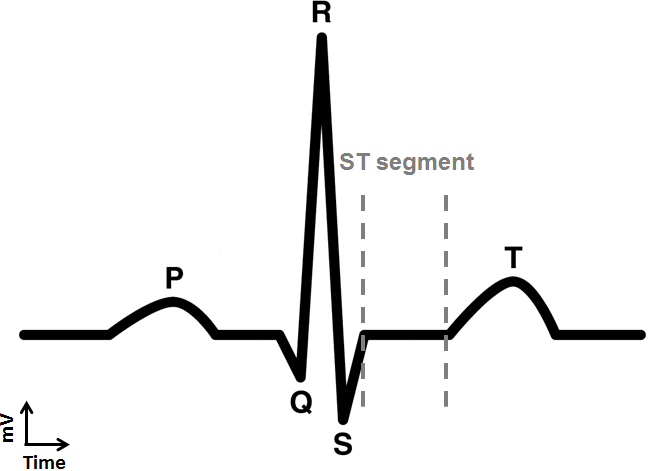
Each heartbeat is controlled by an electrical signal which
travels through the heart, causing the muscle to contract,
pump blood around the body and relax in time for the next
beat. By placing electrodes on a person's chest and limbs,
this electrical activity can be detected and plotted (normally in
millivolts [mV] as a function of time) to form an ECG. As
shown in the diagram (right), the ECG cycle representing one
heartbeat consists of a series of waves (P, QRS and T) with
corresponding segments and intervals, which map the
electrical signal as it travels through the heart. The standard
12-lead (waveform) ECG is typically recorded over a 10-second period so
that many cycles (hence
heartbeats) are recorded. Alterations in the normal ECG recording (changes
in the shape of waves
or the length and height of segments or intervals) might indicate
abnormalities and can be used to
diagnose disorders associated with abnormal heart rate and rhythm,
enlarged heart (hypertrophy)
or heart attacks. However, accurate detection of ECG abnormalities
requires a clear appreciation of
the normal limits of the ECG signal in apparently healthy populations.
The Glasgow Program: key advances since 1993
Professor Peter Macfarlane and his team at the University of Glasgow have
an extensive track
record in ECG research and pioneered the development of automated analysis
and interpretation
of the ECG. By the early 1980s, the team had developed a basic computer
algorithm called the
'Glasgow Program', which could automatically detect ECG components,
compare these with
reference `normal' values and provide an interpretation to aid the
clinical diagnosis of heart
problems. From 1993 onwards, the team has systematically studied the
effects of age, sex and
race on the normal limits of the 12 lead ECG and refined criteria so that
ECG signals can be
accurately interpreted in different patient subpopulations, e.g. males,
females, Caucasians,
Chinese, Africans. The current form of the Glasgow Program incorporates
these refined criteria.
Heart attacks are associated with a characteristic change in the ST
segment on an ECG recording
and consequently the height of the ST segment is used to diagnose heart
attacks. Joint guidelines
issued by the American College of Cardiology (ACC) and European Society of
Cardiology (ESC) in
2000 stated a common diagnostic upper limit for the ST segment height in
most of the 12 leads for
all adults, regardless of age, sex or race. Between 1993 and 2000, the
University of Glasgow team
defined age-based and sex-based criteria for evaluating the height of the
ST segment in the adult
12-lead ECG. In 2001, Macfarlane reported findings obtained through the
examination of ECGs
from 1,338 healthy men and women (age range between 18 and 78 years).
These showed that the
upper limit for the normal ST segment's height in three specific chest
leads was at least 50% higher
in men than in women, and for one of these leads, the upper limit was
distinctly different from the
other two in both men and women.1 The latter finding
demonstrated that this lead should be
evaluated independently of the other two leads when defining the
diagnostic criteria for heart
attacks. Furthermore, the work revealed an age-dependent decrease in the
upper limit in two of
these leads, which is observed only in men. These findings were
incorporated into the existing
Glasgow Program to produce an enhanced version for reporting ST elevation
MI (STEMI).
Validation of the enhanced Glasgow Program's sensitivity and
specificity for diagnosing
heart attack
In a collaborative research study with the medical device manufacturer
Medtronic Physio Control,
the Glasgow team compared almost 3000 ECG recordings taken from Scottish
and American men
and women (approximate age range 20-80 years, 60% of whom had presented
with chest pain)
using either the enhanced Glasgow Program or the 2000 guideline criteria.
The results showed that
the Glasgow Program significantly improved the sensitivity and specificity
of the ECG-based
diagnosis of heart attacks.2 In 2010, the enhanced Glasgow
Program's ability to accurately
diagnose a heart attack was comparable to that of specialist cardiologists
and, in fact, it proved to
be superior in its ability to reduce the number of false-positive
diagnoses.3
The University of Glasgow researchers also provided vital data on
paediatric ECGs by
characterising recordings of over 1,700 healthy neonates, infants and
children.4 This study
revealed that the components of the ECG (particularly the QRS height)
change over the course of
the first few days of life. These findings led to the incorporation of
age-adjusted normal limits for
ECG values in neonates, infants and children into the Glasgow Program.
Use of the Glasgow Program in large-scale clinical trials
The Glasgow Program has been at the design core of a number of
high-profile cardiovascular
randomised clinical trials. The value of combining automated
interpretation with automated coding,
using an internationally agreed scheme, was first demonstrated in the
landmark West of Scotland
Coronary Prevention Study (WOSCOPS).5 As part of this, the
participants' ECGs were recorded
annually for a minimum of 5 years in various health centres in the west of
Scotland, and the
recordings were transmitted electronically over the telephone network to a
central computer for
automated analysis using the Glasgow Program. In this way, the Glasgow
Program detected heart
attacks of which the participants had been unaware. In addition, the ECGs
were automatically
coded using an internationally agreed scheme known as the Minnesota Code.
This approach is
accepted worldwide by epidemiologists as a standardised method for
classifying ECG waveforms.
WOSCOPS highlighted the potential of this approach to control for
variation in ECG-based
diagnosis of heart attacks between clinicians within the same trial centre
and those who are
physically separated on different sites/countries thereby improving the
trial outcome assessment.
Key University of Glasgow researchers: Peter Macfarlane
(Professor in Medical Cardiology
[1991-1995]; Professor of Electrocardiology, [1996-2010]; Honorary
Research Fellow [2010-
present]); Brian Devine (Software Development Manager [1988-present]);
Elaine Clark (Software
Applications Specialist [1998-present); WOSCOPS study group members (see
article for full
details). Key external collaborators: Medtronic Physio
Control
References to the research
Details of the impact
The ECG is used routinely in medicine to assess the health status of the
heart. In addition to
routine monitoring of heart function (e.g. in the general practice setting
or prior to surgery), the ECG
can provide critical insights into various clinical conditions, such as a
heart attack, disorders of
heart rhythm or an enlargement of the heart (as seen in heart failure).
However, the interpretation
of the ECG is complex and requires the reader to have knowledge, skill and
practice to undertake
the task accurately. The University of Glasgow's wealth of research on the
normal ECG, showing
the differences associated with age, sex and race, particularly on the
height of the ST segment,
has driven the revision of clinical guidelines defining the ECG criteria
for diagnosing heart attacks.
Influencing international guidelines on heart attack
An ECG is considered to be the single most important clinical test
in the rapid, initial evaluation of
patients experiencing chest pain due to suspected myocardial infarction
(heart attack). In 2009,
Macfarlane was one of 10 experts who revised the joint recommendations of
the American Heart
Association (AHA), the American College of Cardiology and the Heart Rhythm
Society. The revised
guidelinesa directly adopted Macfarlane's findings published in
2001, which defined different ST-height
thresholds for men and women and stipulated two sets of age-based
thresholds among
men.1 In 2012, the AHA joined the World Heart Federation and
the European Society of Cardiology
(ESC) to publish the `Third universal definition of myocardial
infarction'.a In this guideline, the ST
segment elevation thresholds for diagnosing heart attacks are again based
directly on the
University of Glasgow's work (Table 3 in the document and reference 38).
This consensus
guideline from the leading global cardiovascular authorities is the most
powerful guidance currently
available to cardiologists and standardises the diagnosis of heart attack
around the world.
Commercial adoption of the Glasgow Program by the medical devices
industry
Correct interpretation of the ECG, particularly in the ambulance or the
accident and emergency
department, is usually the basis for immediate treatment
and/or subsequent diagnostic tests.
Whilst cardiologists are expert at interpreting the ECG, these specialists
are not readily available in
all clinical settings. Automated ECG interpretation provides a solution to
this problem.
The global market for ECG monitoring systems is estimated to reach more
than US$800 million in
the next few years. Coupled with the rising incidence of heart disease,
there is a highly lucrative
market for automated ECG interpretation software. The Glasgow Program is a
major competitor in
this market and remains at the cutting edge of electrocardiographic
research. As such it has been
adopted commercially by some of the world's leading electro-medical device
manufacturers in
various product formats, all of which have gained approval from the FDA.
Firstly, the Glasgow Program has been integrated into ECG machines that
acquire, read out and
interpret ECGs. Cardiac Science, a US-based market-leading company with
customers in over 100
countries worldwide, offers this type of product through its Burdick
brand [models 8300 & 8500].
Mindray, a leading Chinese medical device manufacturer, now uses the
program in its R3
electrocardiograph. Secondly, the Glasgow Program has been embedded
into computer software
packages that accompany Holter monitor ECG systems: Telemed Solutions'
flagship product is the
TM-12 recorder. Thirdly, Draeger use the software in its patient
monitoring system — the Infinity®
Central Station. Finally, the Glasgow Program has been combined with
defibrillator/patient monitor
devices such as the Physio-Control Lifepak®15.b
Physio-Control states that:
"It is important that our product use an ECG analysis program that is
widely used in clinical
practice and is recognized as being among best in class. The Glasgow
program meets those
requirements. The Glasgow program gave us an advantage over our previous
generation
product in that the Glasgow program adjusts its STEMI criteria based on
patient gender and,
for men, on patient age." — Principal Scientist, Physio-Control Inc.c
[text removed for publication]. Inclusion of the Glasgow Program in the
above devices allows faster
recording and immediate interpretation of ECGs, thereby reducing, and even
eliminating, the need
for routine manual ECG interpretation and filing. The read-out format of
the Program contains
headline statements (such as `CONSIDER ACUTE STEMI' and `SIGNIFICANT
ARRHYTHMIA'),
which can aid initial diagnosis. Such headline statements are especially
important for emergency
ambulance services, which need to decide quickly whether a patient should
be taken to a heart
specialist centre, for example. Furthermore, the Glasgow Program is one of
the few automated
systems that can accurately interpret ECGs from birth, thereby enabling
clinicians to use this
diagnostic tool in a paediatric setting.
Since 2008, over 40,000 devices containing the Glasgow Program have been
sold worldwide to a
range of end-users.d For example, Physio-Control has sold a
significant number of Lifepak®15
devices to UK ambulance services, including around 740 to the
London Ambulance Service (LAS).c
LAS responds to an estimated 1.5 million emergency calls per annum and has
reported an
increase in survival following a cardiac arrest from 12% to 32% in the
last five years. It is
conceivable that the rapid and reliable interpretation of ECGs with the
Glasgow Program will have
contributed to this improvement.e Similarly, Physio-Control
Inc. has sold devices to fire services as
well as other medical service vehicles, ships and hospitals.c
As each of these 40,000 devices will
undoubtedly be used on multiple patients, the software is estimated as
being used to interpret the
ECGs of millions of patients annually.
Influence on practice-changing clinical trials and epidemiological
studies
The Glasgow Program has been used in a number of large multi-centre
randomised controlled
clinical trials and epidemiological studies. The dedicated University of
Glasgow Core Labf acts as a
partner to a number of stakeholders in clinical trials by providing a
standardised approach to ECG
interpretation that is used in all centres. Since 2008, the Glasgow
Program and Core Lab have
been involved in over 12 trials and studies. These trials have established
major clinical outcomes of
international significance, for example the benefits of statins in
preventing cardiovascular disease,
which have themselves led to changes in guidelines and clinical practice.
Sources to corroborate the impact
a. International guidelines
b. Medical device companies citing inclusion of the Glasgow
Program in their product:
Cardiac Science — Burdick 8300 ECG and Burdick 8500 ECG
(until mid-2013 available directly
from Cardiac Science, now sold via distributors e.g. Moore
Medical Burdick 8300 ECG and
Fisher
Medical Burdick 8300 ECG); Mindray — R3
electrocardiograph; Telemed Solutions — TM-
12
recorder; Draeger — Infinity®
Central Station; Physio-Control — Lifepak®15
monitor/defibrillator
device (`Interpretive algorithm' section, p17)
c. Statement from Principal Scientist, Physio-Control Inc. available on
request
d. Commercial adoption of the Glasgow Program
- Full list of medical device companies who have purchased or extended
rights to use the
Glasgow Program since 2008 is as follows: Schmidt, McKesson,
Cardiolex, Cardiac Science,
Draeger, Epiphany, Heartlab, Spacelabs Healthcare Inc., Physio-Control
Inc., Dan Medical,
AMPS, Mindray Inc., Memtec Corporation (who licence to Telemed
Solutions), Vitalograph Ltd.,
Allengers, Gestio Agfa, Mediana Co., Maestros Mediline Systems Ltd.,
Quinton.
e. Physio-Control `Inside
Physio' website. The link at the bottom of this page `Click here
to read
about LAS' redirects to a PDF document `LAS NHS Trust: A model
system of care' confirming
enhanced survival rates (p1) and 740 devices purchased (p3).
f. ECG
core lab, a service for large multi-centre clinical trials.